
From the 1Department of Neurobiology, Care Sciences and Society, Division of Physiotherapy, Karolinska Institutet, 2School of Education, Health and Social Studies, Dalarna University, 3Functional Area Occupational Therapy & Physiotherapy, Allied Health Professionals Function, Karolinska University Hospital, Stockholm, 4Pain and Rehabilitation Centre, and Department of Health, Medicine and Caring Sciences, Linköping University, Linköping, and 5Center for Clinical Research Dalarna - Uppsala University, Falun, Sweden
Objective: To investigate prognostic factors for physical and emotional functioning following interdisciplinary multimodal pain rehabilitation, by targeting patients’ baseline characteristics and health measures.
Methods: A prospective cohort of 2,876 patients from 38 specialist clinics across Sweden, who were completing interdisciplinary multimodal pain rehabilitation programmes, was followed through the Swedish Quality Registry for Pain Rehabilitation, from initial assessment to 12-month follow-up. Using logistic regression, baseline data were regressed to predict improvement in Physical functioning and Emotional functioning, derived from principal component analyses of the 36-item Short Form Health Survey (SF-36) and the Hospital Anxiety and Depression Scale (HADS).
Results: Employment status emerged as having the largest effect sizes in both Physical functioning and Emotional functioning; Working: odds ratio (OR) 2.05 (95% confidence interval (95% CI) 1.64–2.56) and OR 1.59 (95% CI 1.27–1.98), respectively. Strong beliefs in restored health, better initial emotional health, lower levels of pain and pain interference, and younger age all predicted Physical functioning. European origin, higher levels of general activity, and sense of life control all predicted Emotional func-tioning. Worse initial physical and emotional health predicted the corresponding dependent outcomes.
Conclusion: Employment was consistently found to be an important prognostic factor, suggesting the significance of avoiding delay in interdisciplinary multimodal pain rehabilitation. A positive treatment expectancy was of importance. In general, multidimensional measures indicated that better initial status was more favourable; however, inconsistency implies a complex prognostic picture.
Key words: chronic pain; multidisciplinary pain clinic; prognosis; registry; treatment outcome; health-related quality of life.
Accepted Jan 15, 2020; Epub ahead of print Jan 28, 2020
J Rehabil Med 2020; 52: jrm00019
Correspondence address: Elena Tseli, Department of Neurobiology, Care Sciences and Society, Division of Physiotherapy, Karolinska Institutet, 23100, SE-141 83 Huddinge, Sweden. E-mail: elena.tseli@ki.se
Chronic pain is a common condition that negatively affects most areas of a persons’ life and is difficult to alleviate. Research indicates that interdisciplinary multimodal pain rehabilitation is effective in improving physical and emotional functioning, but little is known about the prognostic factors for a good treatment outcome. Therefore, this study investigated how different patient characteristics related to these outcomes, by following 2,876 patients across Sweden over a 1-year period. It was found that patients who were either currently working or on short-term sick leave clearly had a better prognosis in both outcomes than those with a longer time off from work. In addition, positive treat-ment expectations, levels of emotional health, and coping strategies played an important role, but were not consistent for both outcomes, suggesting a complex prognostic picture for the overall understanding of improvement. These results emphasize the importance of early intervention before patients are too distanced from the labour market.
It is recognized that chronic pain (CP), defined as pain lasting ≥ 3 months or beyond the point of normal tissue healing (1), is often followed by a distinctive, biopsychosocial complexity beyond the symptom of pain itself. CP is today acknowledged as a disease in its own right, referred to as “chronic primary pain” (2) and is a common problem in the general population. Breivik et al. reported that approximately 19% of the adult population in Europe has CP of at least moderate intensity that has lasted ≥ 6 months (3). Musculoskeletal, non-malignant pain conditions, such as neck and back pain or widespread pain, constitute the majority of CP cases. CP interferes with most areas of life and is associated with poor overall health and an increased risk of mortality, and is therefore considered to be one of today’s leading public health challenges (2–5).
Evidence distinguishes interdisciplinary multimodal pain rehabilitation (IMPR) programmes as the best treatment approach available (6–9). With a biopsychosocial approach and, based on the principles of behavioural therapy, it incorporates patient education and physical and psychological measures, and is often accompanied by measures towards return to work (10). Although the content, the composition, and the prevailing terminology may vary, a common goal of all IMPR is to improve functioning and quality of life despite persistent pain (10, 11). Therefore, when evaluating the efficacy or effectiveness of IMPR, aspects of physical and emotional functioning are essential, along with the more general measures concerning health-related quality of life (HRQoL) (12).
Evaluations of treatment effectiveness have, however, revealed only small to moderate effect sizes (6–9). Knowledge of predictive factors could help identify which patients will benefit, or how IMPR can be more effectively adapted to patients’ limitations and resources; however, the lack of conclusive evidence is still an obstacle to this. Existing studies commonly suffer from lack of power due to small sample sizes, while, on the other hand, systematic reviews with meta-analyses are hampered by large study heterogeneity (8, 9, 13, 14). Several factors have been reported to be associated with, and impact on, the prognosis of treatment effects of IMPR, reflecting a biopsychosocial panorama: pain and interference with everyday life, psychological distress, as well as sociodemographic characteristics (9, 13–18). However, the relative importance of these factors require further validation in studies with large and clinically representative samples.
Pragmatic clinical registry studies have been recommended in rehabilitation research as a powerful and highly cost-effective method of establishing clinical evidence reflecting real-world care (19). Currently, IMPR programmes are offered by nearly all specialist pain clinics in Sweden, all of which are linked to the Swedish Quality Registry for Pain Rehabilitation (SQRP). The SQRP aggregates prospectively collected data on a valid set of outcome domains in accordance with current guidelines (12, 20), with the aim of enabling well-powered, high-quality, longitudinal evaluations of IMPR programmes, using a mandatory set of patient-reported outcome measures (PROMs) reflecting the biopsychosocial complexity of CP.
The aim of the present study was to investigate prognostic factors for 12-month follow-up outcomes in physical and emotional functioning following IMPR in patients with CP. It was hypothesized that several biopsychosocial factors known at baseline would predict clinically important outcomes.
Design and subjects
This study used a nationwide multicentre prospective cohort study design, based on prospectively collected data at specialist IMPR clinics across Sweden, which is routinely forwarded to the SQRP. The SQRP continuously aggregates this comprehensive data from all Swedish IMPR specialist pain clinics, which includes data from patients aged 18–67 with chronic (> 3 months) non-malignant musculoskeletal pain who are referred to any of the affiliated clinics for assessment and rehabilitation; some 6,000 new patients are added each year. Affiliated clinics adhere to national guidelines of IMPR criteria, which indicate that 3 or more professionals practice an interdisciplinary team-based approach. IMPR programmes generally include group activities, such as pain education, supervised physical activity, training in simulated environments, and cognitive behavioural therapy (CBT), all of which are coordinated by an interdisciplinary team (e.g. a team could consist of a physician, occupational therapist, physiotherapist, psychologist, and a social worker). The programmes are run mainly through outpatient clinics and typically last approximately 10 weeks. As indicated, SQRP is based on a valid set of outcome domains and measures in accordance with the recommendations of the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT) (12) and the Validation and Application of a patient-relevant core set of outcome domains to assess multimodal PAIN therapy (VAPAIN) consensus (20). Patients complete the SQRP questionnaires: (i) at the initial assessment (i.e. their first visit to the clinical department), (ii) immediately after completing the IMPR programme (data not analysed here), and (iii) at the 12-month follow-up after the end of rehabilitation, providing data used to define the dependent measures specified below.
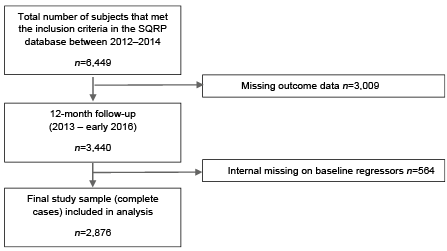
Eligibility for inclusion in the present study was given to patients aged 18–67 years with pain ≥ 3 months, who participated in an IMPR programme between 2012 and 2014 and who took part in the 12-month follow-up between 2013 and early 2016 (until complete 2015 follow-up data was registered), and who had given consent for participation in the SQRP. The present study was based on 2,876 complete cases with CP from 38 specialist IMPR clinics in Sweden (Fig. 1; subject-flow detailed under Results). This study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice and approved by the Ethical Review Board in Stockholm (Dnr: 2013/1842-31/2).
Fig. 1. Flow chart of the selection procedure of the study sample. SQRP: Swedish Quality Registry for Pain Rehabilitation.
Baseline regressors
Eighteen baseline regressors (potential prognostic factors) were used in the initial regression analyses. The variables, which represent sociodemographic, pain-related, and other multidimensional health descriptors, were selected on the basis of clinical relevance and previous evidence, in support of our hypotheses of a biopsychosocial panorama of importance for prognosis, and were as follows:
Patient characteristics. (* marks reference category used in regression analysis): Age: (in years), divided into 3 categories: 18–35*, 36–50, 51–67; reflecting the 0–24th, 25–74th, and 75–100th percentile. Sex: Male or Female*. Education level: Elementary School*, Upper Secondary School, University or College, or Other. Country of origin: Sweden*, Other European country, or Outside Europe. Employment status: Off work, more than one year*, Off work, less than one year, or Working. Beliefs of restored health: Likert scale 1–5 (from 1 = not at all convinced* to 5 = totally convinced).
Pain-related variables. Pain duration (days) was converted into the following categories: 3–12 months*, 13–24 months, 25–61 months, > 61 months based on clinical relevancy. Number of pain regions: ≤ 2 regions*, 3–6 regions, > 7 regions, but not chronic widespread pain (CWP), or CWP. The number of pain regions and their localization was calculated from patients’ ratings on a form with 36 anatomical predefined areas (18 on the left side, 18 on the right side: 1) head/face, 2) neck, 3) shoulder, 4) upper arm, 5) elbow, 6) forearm, 7) hand, 8) anterior aspect of chest, 9) lateral aspect of chest, 10) belly, 11) genitals, 12) upper back, 13) lower back, 14) hip/gluteal area, 15) thigh, 16) knee, 17) lower leg, and 18) foot. The criteria for CWP included checking all 4 anatomical quadrants and the centre of the body, using the American College of Rheumatology classification criteria’s stricter interpretation for CWP (21). The numeric rating scale (NRS) (22) was used to capture the pain intensity of the previous 7 days. The NRS is an 11-point numeric rating scale validated with end descriptors provided for guidance (0 = no pain and 10 = worst imaginable pain) and is analysed here as a continuous variable.
Multidimensional measures (scores were analysed as continuous variables): The Swedish version of the Multidimensional Pain Inventory (MPI) (23) was used to measure pain-related consequences. This study used the pain interference subscale (MPI Pain interference), the life control subscale (MPI Life control), and the Social support subscale (MPI Social support). The general activity index (MPI Overall activity), a composite scale based on 4 subscales, reflecting one’s engagement in common activities of daily life, was also used. The subscales and the index range from 0–6, with higher scores indicating better function for all scales, the only exception being MPI pain interference.
The Swedish version of the Hospital Anxiety and Depression Scale (HADS) (24) was used to measure the level of anxiety and depression. HADS is a 14-item self-assessment questionnaire in which 7 items address anxiety and 7 items address depression (subscales; HADS-D – depression and HADS-A – anxiety). The subscale scores can range from 0 to 21, with lower scores indicating better function (score ≥ 11 points on either set of questions indicates probable anxiety or depression; score 7 or less is considered as a non-case).
The Swedish version of The Short Form Health Survey (SF-36) (25) was used to measure HRQoL. SF-36 is a 36-item self-reported questionnaire in which the items are divided into 8 subscales, representing various health domains, from which 2 indexes can be generated; the Physical Component Summary (SF-36 PCS) and the Mental Component Summary (SF-36 MCS). The SF-36 PCS represents physical health, based on the following subscales: Physical functioning, Role physical, Bodily pain, and General health, while the SF-36 MCS represents mental and emotional health, based on the following subscales: Vitality, Social functioning, Role emotional, and Mental health. The indexes range from 0 to 100, with high values indicating good health.
The Swedish version of the EuroQol-5 dimensions, 3 level version (EQ-5D-3L) (26) was used to measure perceived state of health. The first part of EQ-5D-3L consists of a descriptive system of 5 dimensions; mobility, self-care, usual activities, pain/discomfort, and anxiety/depression with 3 severity levels (no/some/extreme problems). The 5 dimensions can be converted into a summary index (EQ-5D Index), which ranges from –0.594 to 1, where 1 represents “perfect health” and values below zero represent states “worse than death”.
Dependent measures
With the aim of creating composite outcomes, the SQRP data (NRS, MPI, HADS, and SF-36) was examined using principal component analysis (PCA), an effective method for examining underlying constructs summarizing a set of data in a particular study group, therefore reducing the number of possible outcome variables. Our PCA with orthogonal rotation emerged with 2 distinct components, relating to Physical functioning and Emotional functioning, based on the SF-36 PCS solely, and SF-36 MCS, HAD-A, and HAD-D (varimax rotated component matrix: –0.9 and –0,9, 0.8, 0.9), respectively, hence reflecting a wide biopsychosocial perspective on functioning and HRQoL. Neither of the other variables (NRS and MPI) proved suitable for a common factor.
To create discrete binominal outcomes based on a clinically meaningful change, we used the minimal clinical important difference (MCID) as a definition of improvement on our dependent outcomes (27). For Physical functioning, a difference ≥ 3 on SF-36 PCS was regarded as a MCID (28), while for Emotional functioning, at least 2 of the measures in the component were required to attain MCID, one of which had to be SF-36 MCS ≥ 3 (28), and either one (or both) HADS scores, HADS-D ≥ 1.5, HADS-A ≥ 1.5 (29).
Statistical analyses
All analyses were performed using IBM SPSS Statistics for Windows (Version 24.0. Armonk, NY, USA). Descriptive statistics of baseline data were presented with mean (SD), median, or proportions (%), where relevant. Binary logistic regression was initially used to quantify the univariate associations between baseline variables (regressors) and outcomes, and a generous inclusion criteria of p ≤ 0.2 was preferred for further analyses in multiple regression models (30). Potential multicollinearity bias among the regressors was examined by evaluating whether the variation inflation factors (VIF) exceeded 3 for multicollinearity and 1 for tolerance.
Using a top-down approach, the final multiple regression model was identified in a 2-step procedure. Firstly, stepwise backwards elimination was used to eliminate variables based on the highest p-value, until only variables significant at p ≤ 0.2 remained. Secondly, in accordance with the purposeful selection process described by Hosmer et al. (30), variables already eliminated in the univariate analyses were included one by one in the multiple regression model and retained if they were significant at p < 0.05, yielding a preliminary final model with all variables significant at p ≤ 0.2. Baseline regressors significant at p < 0.05 in the final model were recognized as important prognostic factors. All p-values were based on the likelihood-ratio test, and categorized variables were assessed by their overall p-value.
In the results, odds ratios (ORs) and their 95% confidence intervals (95% CI) are presented along with p-values; an OR represents a standardized regression coefficient, where < 1 indicates a negative association with the outcome and > 1 a positive association. The proportion of explained variance by the model was evaluated with Nagelkerke R-square and Cox & Snell R-square and the degree of correct classifications was assessed by overall percentage. To determine the overall precision of the models, i.e. their discriminative ability of true positive outcomes (cases) and true negative outcomes, the area under the curve (AUC) was evaluated using the reference criteria of common guidelines; poor < 0.7, acceptable > 0.7 discrimination (30).
Study attrition and sample characteristics
During the period 2012–14, 13,778 subjects were referred to specialist evaluation at an SQRP-affiliated clinic in Sweden. Of these, 6,849 patients (nearly 50%) were selected to take part in an IMPR programme. Almost all of the patients (n = 6,449) eventually participated in an IMPR programme; however, 393 discontinued their programme and information on participation was missing for 7 patients (see patient flow in Fig. 1). The reasons for discontinuing IMPR programmes were either due to the patient’s own decision (n = 219), need of other medical service (n = 105), or other unspecified reasons (n = 69). At the 12-month follow-up after the programme, 3,440 patients (53%) had reported complete data on the dependent outcomes SF-36 and HADS. The remaining 3,009 patients (47%) had missing outcome data and were therefore not included in the analysis. Due to internal missing data in any of our listed baseline regressors, an additional 564 patients (9%) were excluded from the analysis. Details of sociodemographic characteristics and baseline status for patients included and for those with any missing values are shown in Table I. When comparing these complete cases vs those with missing data for a number of variables (as listed in Table I), a few differences were found, indicating that a larger proportion of the patients with missing values were born outside Europe and had a lower degree of vocational connection.
Table I. Personal characteristics and baseline data for included and excluded (missing data) patients
Hence, a total of 2,876 patients were included in the final analyses, the majority of whom were women (77%). The current pain intensity was reported to be 7 on a 0–10 numeric rating scale, and in most cases pain had persisted for > 5 years. Moreover, regarding HRQoL, the mean ratings on physical and mental health did not precede 40 (scores below 50 is considered below the population mean) on the 0–100 scale of SF-36 PCS and SF-36 MCS, respectively, and levels of emotional distress indicated possible cases with mean scores above 8 on HADS-A and HADS-D, respectively.
At the 12-month follow-up, 50% of patients had attained an improvement (equivalent of ≥ 1 MCID) in either one dependent variable, Physical functioning or Emotional functioning, or both (21%), rendering a total of 71% of patients attaining an improvement on any of these 2 dependent variables, while 29% did not improve on our MCID.
Univariate analyses
For Physical functioning, 14 regressor variables were associated with improvements and reached the entry level for further analyses: 4 personal characteristic variables, 2 pain-related variables, and 8 multidimensional variables, all highlighted in bold in Table II. For Emotional functioning, 12 regressor variables were correlated with improvements, and also reached the entry level for further analyses: 3 personal characteristic variables and all 9 multidimensional variables (see Table III).
Table II. Univariate logistic regression analysis of improvement in Physical functioning at 1-year follow-up after an interdisciplinary multimodal pain rehabilitation programme
Table III. Univariate logistic regression analysis of improvement in Emotional functioning at 1-year follow-up after an interdisciplinary multimodal pain rehabilitation programme
Multiple logistic regression analyses
After the stepwise reduction, 8 and 5 regressors remained in final models for Physical functioning and Emotional functioning, respectively (Table IV). For Physical functioning, Employment status proved to be a significant prognostic factor for improvement: Working at baseline and time off work < 1 year were both significantly associated with improvement, compared with time off work > 1 year (OR 2.05, 95% CI 1.64–2.56 and OR 1.65 95%, CI 1.26–2.15, respectively). Also, one’s belief in restored health emerged as an increasingly important predictor for improvements (totally convinced of restored health: OR 2.43, 95% CI 1.77–3.33). Higher emotional functioning (SF-36 MCS: OR 1.02, 95% CI 1.01–1.03) was also positively associated, as were 5 additional variables: younger age, lower initial levels of pain intensity (NRS), and pain-related interference (MPI Pain interference) in everyday life in conjunction with a lower level of physical functioning (SF-36 PCS), and higher initial levels of anxiety (HADS-A). No interactions emerged. In the final model, the overall percentage of correctly classified cases was 64% and the explained variance 15%, Nagelkerke R-square, 0.151 (Cox & Snell R-square 0.114). Diagnostic tests of the final model indicated acceptable discrimination (AUC 0.70, 95% CI 0.68–0.71).
For Emotional functioning, Employment status proved again to be prognostic of improvement: Working at baseline and time off work < 1 year were both significantly associated with improvement, compared with time off work > 1 year (OR 1.59, 95% CI 1.27–1.98 and OR 1.62, 95% CI 1.24–2.13, respectively). A lower level of emotional health (SF-36 MCS) emerged as correlated (OR 0.92, 95% CI 0.92–0.93), as were 3 additional variables: a European origin, higher overall activity levels (MPI Overall activity), and higher sense of life control (MPI Life control). In this final model, the overall percentage of correctly classified cases was 67% and the explained variance 21%, Nagelkerke R-square, 0.210 (Cox & Snell R-square 0.157). Diagnostic tests of the final model indicated fair discrimination (AUC 0.73, 95% CI 0.71–0.75).
Table IV. Multiple logistic regression analyses of improvement in Physical and Emotional functioning at 1-year follow-up after completion of an interdisciplinary multimodal pain rehabilitation programme
This study investigated prognostic factors for 12-month follow-up outcomes in Physical functioning and Emotional functioning. The major results were:
Employment status as a prognostic factor
These results showed that proximity to employment was the most important predictor for a positive prognosis for both Physical functioning and Emotional functioning. These findings are consistent with studies reporting that working at the initiation of IMPR favoured improvement in HRQoL (31), pain intensity (16), disability (32), and return to work (33). Employment therefore seems to act favourably for several intended IMPR outcomes. It has been claimed that being unemployed or receiving long-term benefits is a source of high socioeconomic stress, which can be a barrier to rehabilitation success (34, 35). The current results also indicated that longer periods away from work are associated with poorer outcomes. This underlines the significance of the timeline before IMPR, as the negative effect progressed over time suggests that efforts should be taken to avoid delaying the start of IMPR. Finally, working and contributing towards society is correlated with higher levels of HRQoL and lower levels of emotional distress, since the workplace is an important arena for self-affirmation (36) and is consequently in itself an objective to strive for.
Resilient psychological factors favour a good prognosis in physical functioning
Optimistic thoughts about health being restored played an important part in a person’s chances for a positive outcome in Physical functioning; the higher the expectations the better the prognosis. The influence of such an expectancy on outcome has been recognized in several therapeutic fields (37), including CP rehabilitation (16, 38, 39). Goossens et al. (39) showed that pre-treatment expectancy was a significant predictor of 1-year outcomes relating to activity, emotional distress, and quality of life, and a study by Gerdle et al. (16) of SQRP data also found similar results. Using a comparably large sample, Cormier et al. (38) also showed that strong positive expectations were linked to superior treatment gains in multiple outcomes, with the exception of depressive symptoms, which resembles the findings of the present study where the favourable effect did not appear for the outcome Emotional functioning.
We also found that for a positive outcome in Physical functioning, better initial emotional health was important. This was also the case for pain intensity and pain interference, both indicating that less is better. All of the above-mentioned baseline characteristics seem to reflect a clinical presentation of the less burdened patient, the “better” the patient entering the IMPR, the better the prognosis, where the optimal baseline prerequisites indicate access to emotional and cognitive behavioural coping resources. A recent meta-analysis on prognostic factors for physical functioning, which aggregated analogous cognitive-behavioural factors relating to optimism, sense of control, and self-efficacy, found that these factors were strongly associated with a better physical functioning at follow-up (18). Hence, our results reinforce earlier findings that emotional health and positive cognitive behavioural factors are indeed important predictors for better physical functioning at follow-up.
Poor emotional status in favour of a good prognosis for emotional functioning
Emotional functioning was mainly predicted by a low baseline status, i.e. poor initial emotional health. This finding is in line with current evidence (15); however, 2 regressors emerged as favourable in this clinical picture; perceived life control and overall activity level, both of which indicated that “higher” levels were related to a good prognosis.
On a general note and similar to previous studies, the baseline levels of Physical functioning and Emotional functioning predicted their corresponding dependent outcomes, where a lower initial level predicted a positive outcome. Similar results have often been interpreted as an effect of regression to the mean, or to the circumstance that the worse your problem is on a certain measure the more likely it is that you may benefit from treatment on that same variable. Our results on this are in agreement with other recent prediction studies that also emanated from SQRP data, where a general pattern indicated that the largest improvements in levels of functioning and life impact of pain were associated with lower initial scores (15, 16).
A complex clinical presentation
The most advantageous patient profile for a positive outcome in Physical functioning, i.e. “better in better out”, appears to be quite different from that for improvement in Emotional functioning, where the clinical presentation is more in line with common perceptions of worse baseline levels being more favourable. Parallel to this, for a positive outcome in Emotional function-ing, some coping factors relating to a higher general activity level and sense of control in daily life were also of importance. Therefore, although the clinical presentation and the prognostic value and direction of some characteristics appear complex, at least those referring to coping and life impact seem to go in the same direction; the better the coping resources, the better the odds of a positive outcome. This further adds to the focus on targeting ways to enhance positive emotions and resilience as a means of improving overall functioning in CP (40).
Strengths and limitations
The cohort used in this study was considered to be a representative sample of the population of people with CP seeking specialist care in Sweden. The demographic characteristics were similar to other cohorts of patients with CP participating in comprehensive IMPR programmes across Europe, and the Western world in general (6, 13, 14, 18). The external validity, therefore, extends to patients with CP referred to and participating in specialized IMPR programmes, targeting the biopsychosocial consequences of the disease.
A strength of this study was the large sample size with national coverage. A relatively high proportion (47%) of patients was lost to follow-up, which is similar to earlier studies with long-term follow-ups (18). A crude missingness analysis showed that the non-responders were similar to the responders on all pain characteristic variables and self-rated health measures; however, a larger proportion of the non-responders were born outside Europe and had a somewhat lower degree of vocational connection, which may partly indicate that information on study participation and questionnaires were not successfully adapted for foreign participants. We used a wide array of well-tested, standardized assessment tools, both generic and disease-specific, covering biopsychosocial domains targeted by modern IMPR programmes (12). In our operationalization of the dependent variables Physical functioning and Emotional functioning, we aspired to use maximum information from plural variables using PCA, i.e. we aimed to reduce the dimensionality of our SQRP data, which consisted of a number of interrelated measures. Also, for the dichotomization of outcomes and the definitions used for improvement we used previously reported MCID definitions (28); however, to our knowledge these are not yet comprehensively validated in patients with CP, which suggests that some attention is required to what a good outcome represents using MCID.
Although many independent measures were included, reflecting sociodemographic, pain-related, cognitive-behavioural, and psychological domains, the degree of explained variance in final regression models did not exceed 21%, indicating that for the complete prediction of outcome much still remains unrevealed. It is suggested that treatment-related regressors, such as treatment duration and treatment content, should be further studied for their effect and prediction power.
Implications and future directions
The favourable effect of retaining a connection to employment was the most evident finding in this study. It appears that, even for patients with a relatively severe clinical baseline status, the work connection is indicative of a better prognosis. This highlights the importance of the timeline and of avoiding delay in starting IMPR, and acknowledges work participation as an important facilitator to provide basis for rehabilitation success. Future studies should also focus on including other aspects of what work connection actually represents; for instance, whether it is the stress relief that enables better dedication to the rehabilitation process or whether this relates more to social participation factors.
The second evident finding in this study was the prognostic value of treatment expectations, where those who believed in restored health had more than doubled odds of reaching a positive outcome in Physical functioning compared with those with low beliefs in restoration, indicating a strong impact of optimistic thoughts on improvement. This implies that, in clinical practice, there could be increased benefits from expectation optimization, e.g. by informing the patient about the expected benefits of a treatment, explaining the suggested mechanisms underlying these beneficial treatment effects, and emphasizing the increase of personal control over the pain condition (37). As indicated, we believe that future studies should also study treatment-related factors in detail, and how these will interact with personal characteristics; perhaps such an approach will result in increased explained variance in the regressions and provide more relevant information to the clinics. In addition, more specific assessments of physical functioning (both patient-reported and objective measures) should be included in national quality registries, as a complement to the existing PROMs.
Conclusion
The results of this study indicate that employment, or only a short period off work (< 1 year), is important for a better Physical functioning and Emotional functioning one year after the completion of an IMPR programme. This indicates an important timeline, suggesting that providing IMPR in the early phases of CP is beneficial. Results also showed how optimistic thoughts and other cognitive-behavioural coping resources were of prognostic value for improvement, especially in Physical functioning. This indicates potential benefits of targeting those variables further for modification in treatment. Importantly, the clinical presentation of importance for improvement differed between the 2 outcomes, where some indicate “better in better out” and others indicate worse baseline levels being more favourable, presenting a complex prognostic picture for the complete understanding of good clinical follow-up.
This study was supported by grants from the Swedish Research Council (2015-02512), Stockholm, Sweden, The Doctoral School in Health Care Sciences, Karolinska Institutet, Stockholm, Sweden, AFA-Insurance (140340), Stockholm, Sweden, The Research-ALF (LIO-608021), County Council of Östergötland, Linköping, Sweden, and The Swedish Research Council for Health, Working Life and Welfare (FORTE; 2017-00177), Stockholm, Sweden. These sponsors had no part in study design, data collection, data analysis, data interpretation, writing of the report, or the decision to submit for publication.


 Click to show fullsize
Click to show fullsize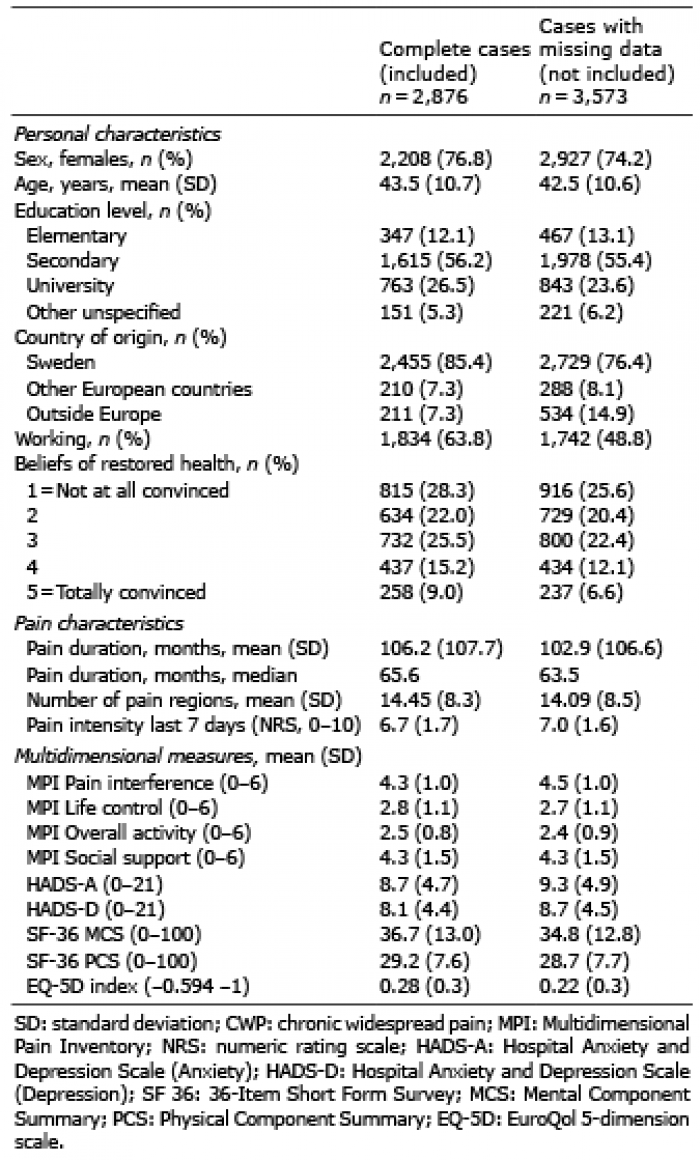 Click to show fullsize
Click to show fullsize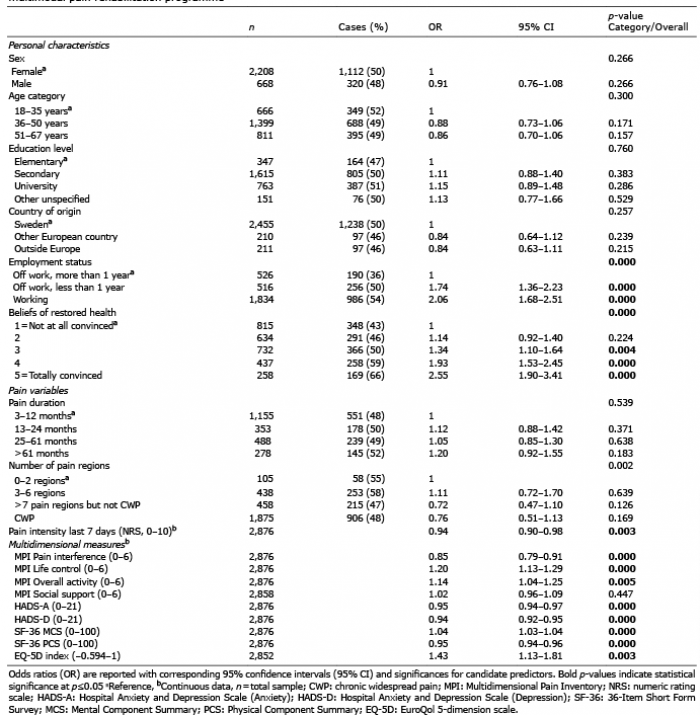 Click to show fullsize
Click to show fullsize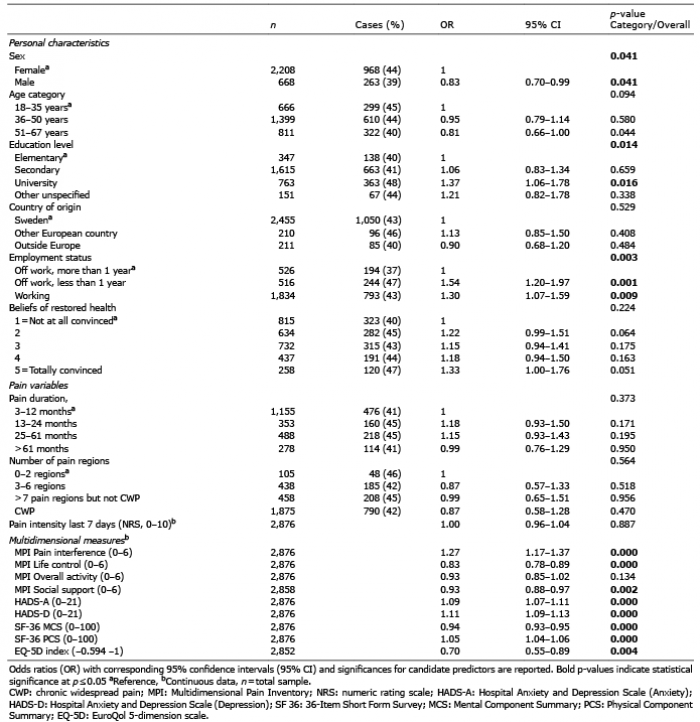 Click to show fullsize
Click to show fullsize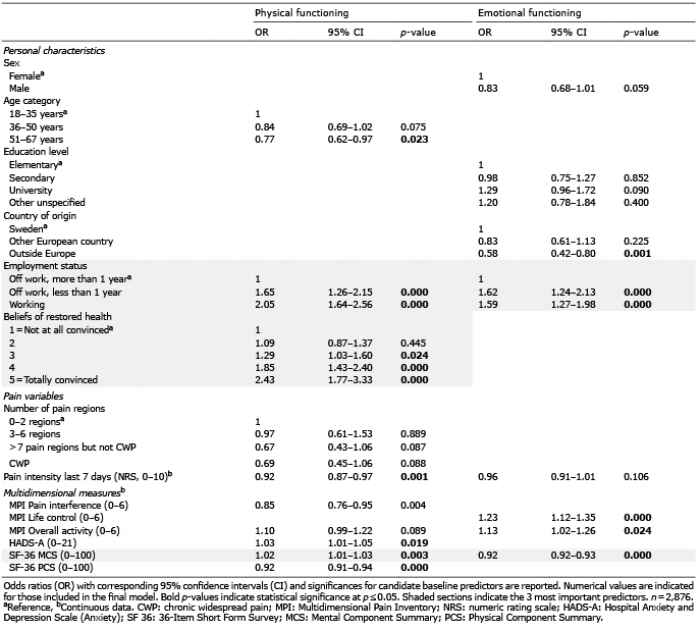 Click to show fullsize
Click to show fullsize